


If my mother gave birth to me today instead of over 60 years ago, she would probably be dead based on her risk factors. She was Black, had gestational diabetes, and gave birth to a 9-pound 4-ounce baby girl via C-section. She would have been discharged from the hospital on post-op day four rather than post-op day seven. But, thank God, my mother, unlike her mother, lived. I never knew my grandmother because she died from postpartum cardiomyopathy at age 39, a few months after delivering my youngest aunt in 1939.
When my mother had me, there were no managed care organizations that booted women out of the hospital 48 hours after birth or 96 hours after having a C-section. Had the federal government not stepped in with the Newborn and Mother’s Health Protection Act of 1996, mothers and babies would have been sent home after 24 hours, a phenomenon sarcastically referred to as “drive-through deliveries.â€
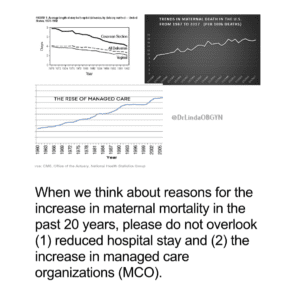
In the discussion of reasons for the ignominious U.S. maternal mortality rates, the topic of managed care organizations and private equity investors is never discussed but should be.
According to Medical Economics, the Medical Management Group Association (MMGA) reported $60 billion in “deals†involving medical practices in 2019 by private equity firms. They are one of the reasons why nurses are leaving hospitals, physicians are jumping off hospital roofs, and yes, women are dying within a week of having a baby, and the stillbirth rate has increased.
The business model is not taught in nursing, midwifery, or medical schools. As a result, we do not know how to compromise quality care and satisfy your shareholders simultaneously. Perhaps if hospital CEOs and private equity shareholders are named co-defendants in future medical malpractice cases, the maternal mortality rate will move in the opposite direction.
You profess not to know why more pregnant women are dying? Try taking a closer look at your priorities and business practices. As long as profit and revenue take precedence over human life, there is little hope for change.

